Uterine Fibroids are the most common benign tumors in reproductive age females. They are not cancerous and can present with or without symptoms. Most of the fibroids are found incidentally on imaging, however 30- 40% of the females with fibroids can be symptomatic.
Risk factors associated with Uterine Fibroid
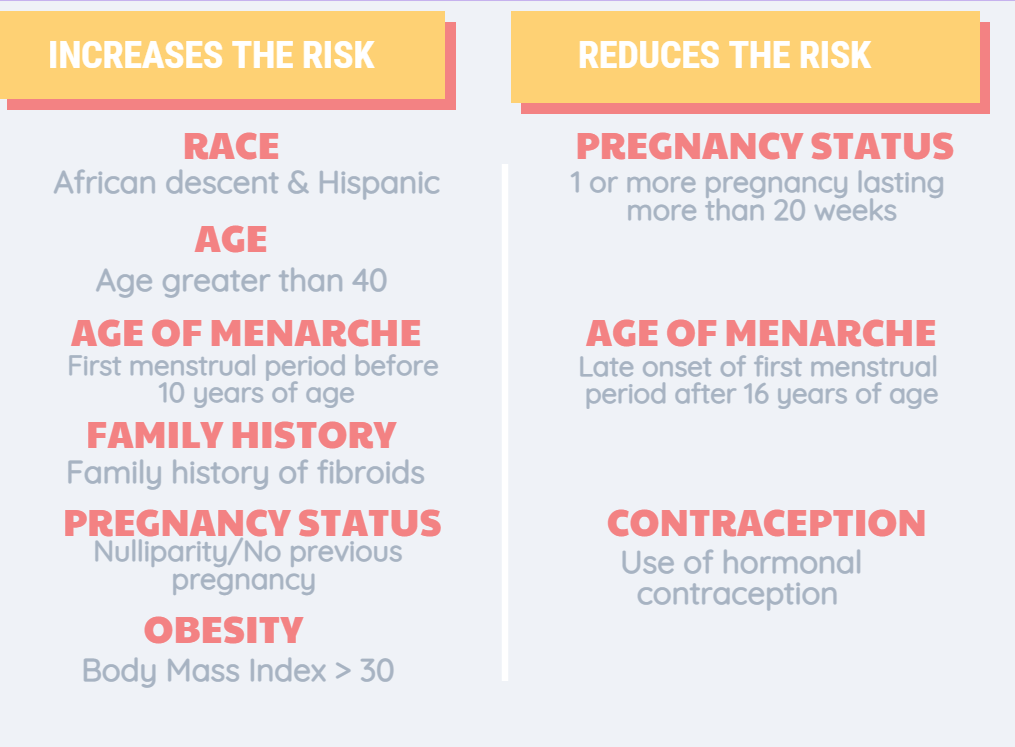
Multiple studies have been performed in the past and have identified certain risk factors to be associated with developing fibroids. African Americans were found to have three times the risk and Hispanic women were found to have two times the risk of developing Uterine fibroids compared to Caucasian women. The risk increases with age in women are in reproductive age and decreases after menopause. Having a family history of Uterine Fibroids increases the likelihood of a women developing it. Studies have shown that early onset of first menstrual period increases the risk of developing fibroids whereas late onset of first menstrual period reduces the risk. Having one or more pregnancy that lasted more than 20 weeks is considered to be a protective factor. similarly being on hormonal contraception protects and reduces the risk of uterine fibroids by managing the hormone production. Obesity can also increase the risk by increasing the estrogen hormone production, which contributes to increase in fibroid size.
Symptoms and presentation
Many women with fibroids can be asymptomatic. However 30 – 40 % of the women with uterine fibroids can present with symptoms. It is important to recognize the symptoms and seek medical help to prevent the fibroids from growing and causing complications.
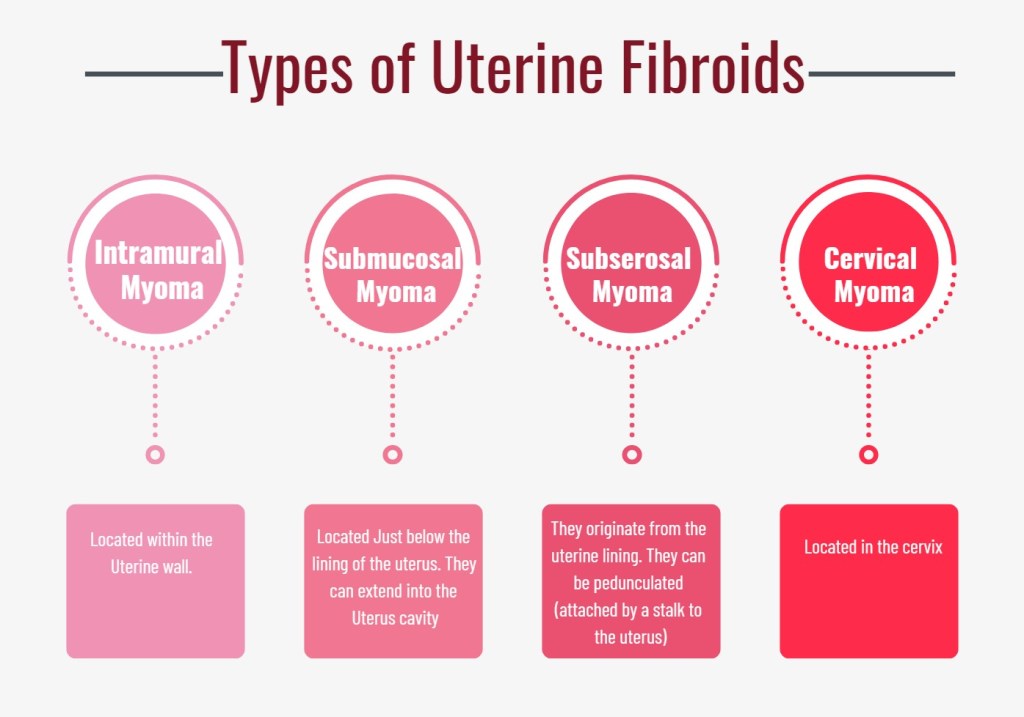
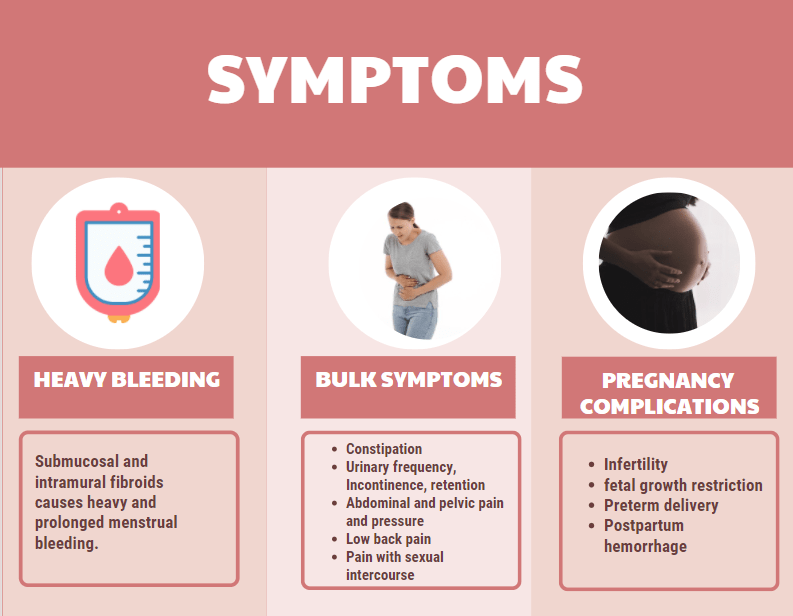
The most common symptoms is heavy or prolonged menstrual bleeding. Heavy menstrual bleeding can also contribute to anemia, fatigue and poor quality of life. The location and type of fibroid determines the quantity of bleeding. Submucosal fibroid that extends into the uterus and intramural fibroid contributes to the most bleeding. Subserosal fibroid do not cause heavy bleeding.
Fibromatous uterus is enlarged and can press on other organs causing other complications such as urinary and bowel abnormalities, low back pain, abdominal and pelvic pressure, painful sexual intercourse. When the enlarged uterus compresses on the bladder it can cause increase frequency of urination, urinary incontinence (leaking of urine) and urinary retention (unable to urinate). Constipation is a very common symptom due to the bowels being compressed. Due to the enlarged uterus and weight of the fibroid and women can feel pressure on abdominal and pelvic area and low back pain. Some fibroids depending on the location can also cause pain with deep sexual intercourse. One can also experience an immediate or acute onset of severe pain due to torsion (twisting) of the pedunculated fibroid that is attached by a stalk to the uterus or from breaking down of the fibroid tissue
Many asymptomatic women were found to have fibroids while being evaluated for infertility. Submucosal or intramural fibroids causes irregularities in uterine cavity and causes difficulty to conceive. Uterine fibroids can also cause complications in pregnancy and during delivery and therefore needs thorough evaluation and additional close care during pregnancy.
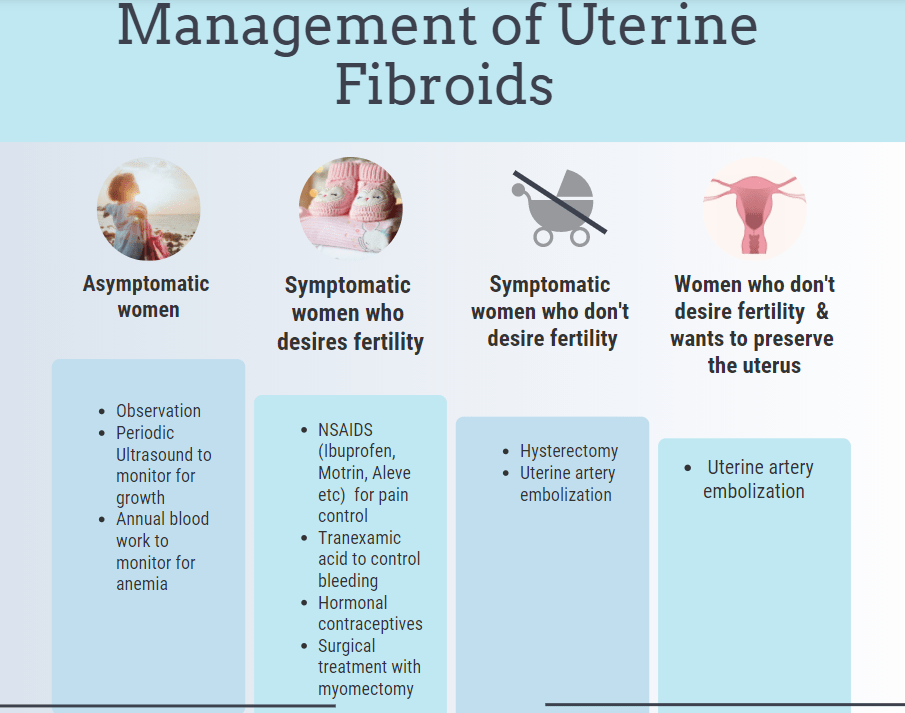
Management & Treatment
For women who are not symptomatic wait and watch approach is safe. Periodic ultrasounds to monitor growth of fibroids and blood work to evaluate for anemia is sufficient in those patients as the fibroids can grow and regress with time.
Treatment options vary based on the size and location of the fibroids, symptoms and desire of future pregnancy. There are medications to simply treat the symptoms such as heavy bleeding and pelvic pain. Tranexamic acid reduces the bleeding without shrinking the fibroids. For pelvic pain NSAIDS such as Ibuprofen, Aleve, Naproxen, Motrin can be helpful. On the other hand there are hormonal contraception medications and devices (Intrauterine device IUD such as Mirena) that can treat the fibroids by shrinking them. Surgical procedures such as laparoscopic or open abdominal myomectomy is used to remove the fibroids and to preserve fertility. Laparoscopic myomectomy is least invasive robotic surgery and is a good option with few risk of complications for few small fibroids. Large , multiple fibroids and submucosal fibroids may need open abdominal myomectomy in which a large abdominal incision is made to open the abdomen to access the uterus. Hysterectomy and uterine artery embolization is a good option for women who do not desire future pregnancy. Uterine artery embolization is suitable for women who do not desire future pregnancy but wants to keep the uterus. It works by discontinuing the blood supply to the fibroid which results in regression of the fibroid.